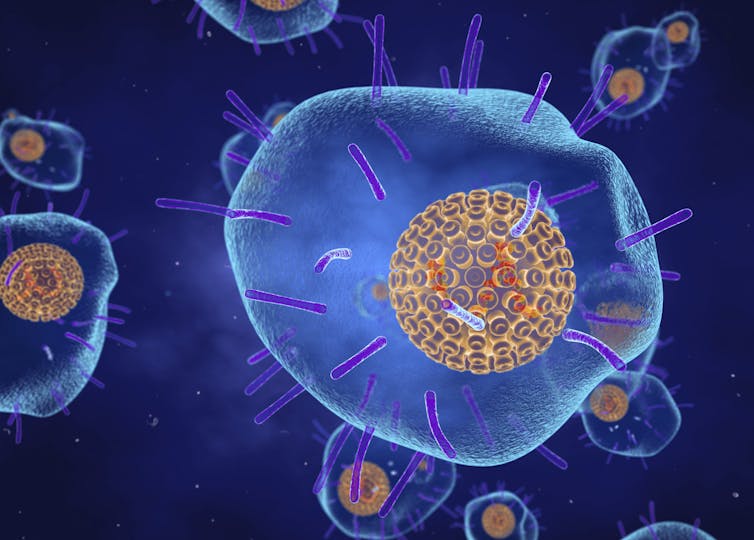
The chickenpox virus has a fascinating evolutionary history that continues to affect peoples' health today
Chickenpox has largely disappeared from the public’s memory thanks to a highly effective vaccine. But the virus’s clever life cycle allows it to reappear in later adulthood in the form of shingles.


In July 2021, a Centers for Disease Control and Prevention presentation obtained by the press noted that the delta variant of COVID-19 “is as transmissible as chickenpox.”
As some researchers have pointed out, the CDC’s comparison was an overstatement. Based on various studies and projections, on average a person infected with the delta strain of COVID-19 can infect six or seven people, whereas someone infected with chickenpox can infect nine or 10. Nonetheless, both diseases are highly contagious, although the viruses that cause them are very different.
While many diseases, such as Ebola and influenza, originate from viruses that made relatively recent “jumps” from animals to humans, other disease-causing pathogens have been with humans throughout evolution. The virus that causes chickenpox is one of these, coexisting with the human evolutionary line for millions of years.
I am a microbiologist interested in pathogens and the diseases they cause. Chickenpox is a childhood disease, and until a couple of decades ago, nearly all children in the United States got it. A vaccine campaign that began in the 1990s has made the disease rare in children in the U.S., but the virus lingers in the body and can reappear in unvaccinated adults years later as shingles. The virus’s ability to do this disappearing-and-reappearing trick may be the key to its long evolutionary history.
Chickenpox and shingles stem from the same virus
I became painfully aware of the virus that causes chickenpox a few years ago when my husband developed shingles soon after starting a stressful job. Chronic stress is one trigger for reactivation of the dormant virus, as it is for the closely related herpes viruses.
The virus that causes both chickenpox and shingles, varicella-zoster, is only known to infect humans. “Varicella” means “little variola,” or little smallpox, because both diseases cause skin blisters.
Shingles is known in medical terms as herpes zoster. Both “zoster” and “shingles” derive from words for belt or girdle in Greek and Latin, respectively, referring to the typical arrangement of blisters on the torso during shingles outbreaks.
Chickenpox is primarily a childhood disease
Chickenpox is spread by inhalation, and children are infectious a few days before symptoms appear. The blisters also contain live viruses that can become airborne and inhaled or can be transmitted through direct contact. After inhalation, chickenpox viruses invade the cells of the respiratory tract, replicate in the lymph nodes and are spread by white blood cells throughout the body. Eventually, they lodge in the skin, causing the itchy blisters that are characteristic of the disease.
In healthy children, chickenpox lasts about a week and goes away without medical intervention. But it can be more severe in adolescents, adults and people with compromised immune systems. Infection with chickenpox typically provides lifelong immunity to reinfection.
Shingles mostly affects older adults
Even after the chickenpox blisters are gone, the varicella-zoster virus is not. The viruses travel to nerve root clusters located along the spinal cord. There, the viruses establish a persistent, dormant state in the nuclei of the nerve cells.
Over the course of a person’s life, the viruses may reactivate, but usually the immune system eliminates the active viruses before they can appear as shingles. However, as the immune system weakens with age, or as a result of illness or stress, reactivated viruses can travel back along the nerves and erupt again as painful blisters. Typically, only one nerve-root cluster is involved, and the blisters appear in the area of the skin supplied by those nerves. This leads to the classic belt-like appearance, although the blisters can localize to other areas of the skin.
Although even children can develop shingles, the risk of that happening and the severity of the disease increases sharply after the age of 50. The CDC estimates that 1 in 3 people in the U.S. will have shingles at some point in their lives. In healthy adults, a shingles outbreak typically lasts from seven to 10 days; however, about 15% of shingles sufferers develop persistent, often debilitating, neurological pain, called postherpetic neuralgia, that can last for months or even years.
Varicella-zoster has a long, slow evolutionary history
Unlike the COVID-19 and influenza viruses, which have genomes of single-stranded RNA, varicella-zoster’s genome is double-stranded DNA. This makes its genome more stable and able to be copied more accurately than single-stranded RNA genomes.
Although experts disagree on the exact rate at which varicella-zoster accumulates genetic changes, called mutations, a reasonable estimate of its evolution rate is one new mutation every 200 to 400 years. This rate is in contrast to influenza, for example, whose RNA genome is copied so sloppily that it accumulates about 40 new mutations every year, according to my calculations based on data published here.
Varicella-zoster is a member of a large group of viruses, the Herpesviridae, that infect mammals, birds and reptiles. Although there have been some “jumps” between hosts in the distant past, these viruses tend to infect only specific hosts. Thus, scientists can deduce the evolutionary history of the viruses by looking at the known evolutionary relationships of their hosts.
Such analyses indicate that the viruses that eventually led to varicella-zoster and its relatives existed 200 million years ago in the Triassic/Jurassic period – the age of dinosaurs! The closest existing relative to varicella-zoster infects an old-world monkey. The evolutionary lines that led to humans and old-world monkeys split 23 million years ago; thus, our cohabitation with varicella-zoster goes back at least that far.
Recent DNA analysis of varicella-zoster strains currently infecting humans complicates this history somewhat. The data indicates that the virus is accumulating mutations faster than would be consistent with its evolutionary history, and that the ancestor of the current strains appeared only about 8,000 years ago. Such discrepancies between short-term and long-term evolutionary rates have appeared in numerous similar studies, and scientists are currently analyzing why this is so.

The ability to enter a latent state may have given varicella-zoster a survival advantage. Ancient hunter-gatherers would have lived in small groups where an outbreak of chickenpox could have infected the whole population. A credible theory proposed by Charles Grose, a pediatric infectious disease specialist at the University of Iowa, holds that, since chickenpox conveys lifelong immunity, the survivors could not be reinfected. And without new hosts, the virus would die out. However, by persisting for years in survivors in its latent state, varicella-zoster could reappear after a new generation of children was born. Since the shingles blisters are infectious, these children would get chickenpox and a new cycle would begin.
Vaccines for chickenpox and shingles are effective
Prior to 1995, when the chickenpox vaccine was introduced, nearly all U.S. children got infected with chickenpox by age 10. Although usually mild, rare complications resulted in more than 10,000 hospitalizations and 100 deaths per year.
The two-dose vaccine has resulted in greater than 90% protection against infection. Currently the vaccination rate among schoolchildren approaches 95%. By preventing the virus from spreading, this level of vaccination protects unvaccinated children through herd immunity.
The chickenpox vaccine is a live, attenuated varicella-zoster strain that, like the original strain, stays in the body in a dormant state. But the vaccine strain is weakened for activation, and as of 2016 data show that children vaccinated for chickenpox develop shingles less frequently than children did when chickenpox was common. Public health experts do not yet know whether the rate of vaccine-derived shingles will rise as the vaccinated population ages and becomes more susceptible to the disease.
Shingrix, an effective, protein-based vaccine against shingles, has been available since 2017. The CDC recommends everyone over age 50 to get vaccinated for shingles, whether or not they have had chickenpox, shingles or have been vaccinated with Zostavax – a former shingles vaccine that was less effective. Shingrix reduces the incidence of shingles an average of 97% and, if a case occurs, reduces the incidence of postherpetic neuralgia by 91%.
Vaccination requires two doses and is known, so far, to be protective for at least 10 years. As of 2018, 34.5% of U.S. adults 60 and over were vaccinated against shingles, most with Zostavax.
With effective vaccines against both chickenpox and shingles now available, I believe that the countries with high vaccination rates could eventually be free of both of the diseases caused by varicella-zoster – ultimately making the chickenpox-shingles duo go the way of the dinosaurs.
[Get our best science, health and technology stories. Sign up for The Conversation’s science newsletter.]![]()
Patricia L. Foster is affiliated with the Union of Concerned Scientists and Concerned Scientists at Indiana University.
What's Your Reaction?